A 2023 study published in the Journal of Cosmetic Dermatology found that fewer than 40% of people who start a retinol regimen stick with it past the three-month mark, largely because of irritation and peeling. That dropout rate tells a real story about the gap between what an ingredient can theoretically do and what most people can actually tolerate in daily life. Meanwhile, peptide serums have quietly become some of the best-selling beauty articles and products on the market, promising similar anti-aging benefits without the redness. So which one is worth your money and your bathroom shelf space?
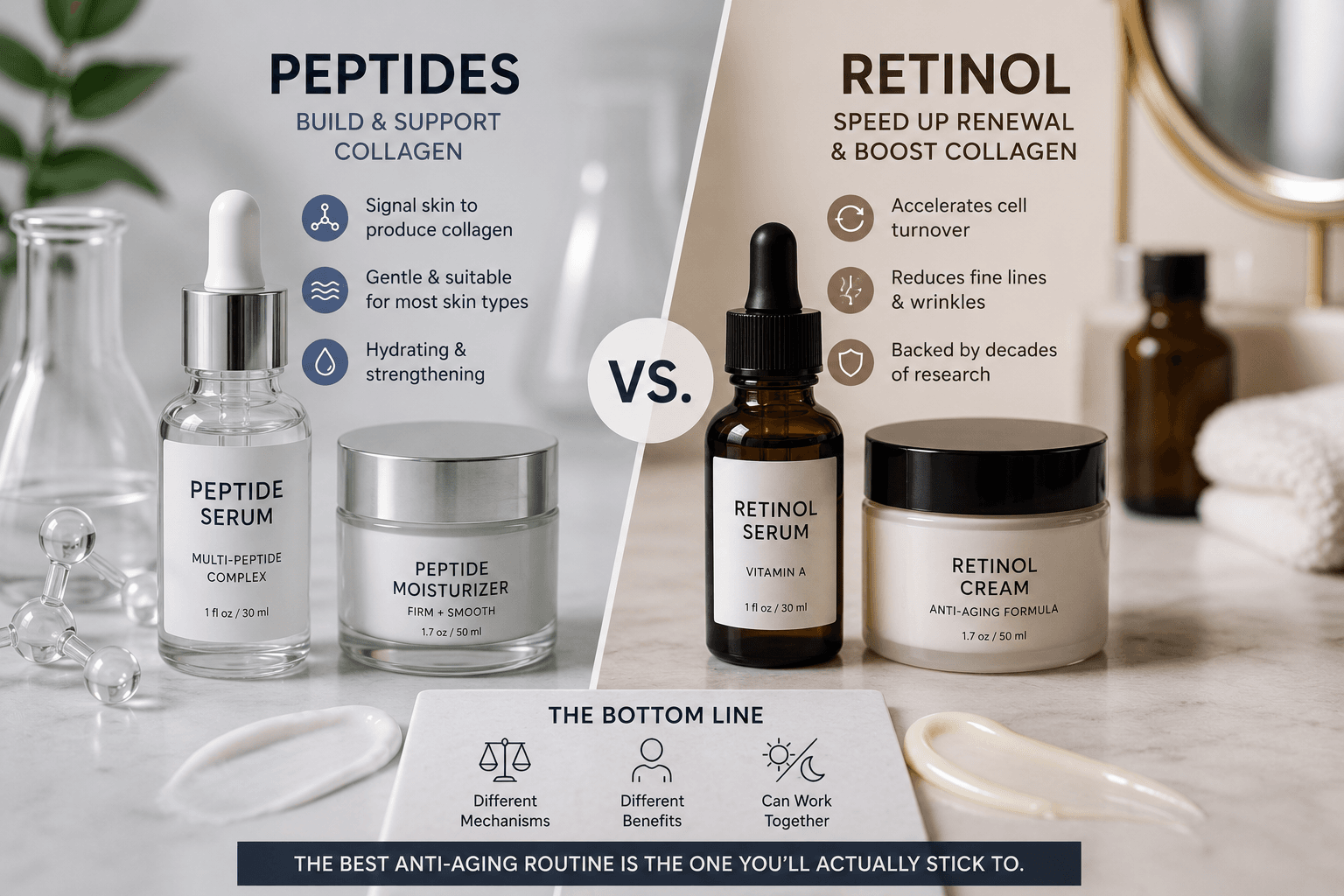
The honest answer is that retinol (retinyl palmitate in its ester form, or retinaldehyde as a step closer to retinoic acid) and peptides work through entirely different biological mechanisms. Retinol has decades of peer-reviewed backing as a gold-standard topical for collagen stimulation and cell turnover. Peptides, short chains of amino acids like palmitoyl tripeptide-1 or acetyl hexapeptide-3, work more gently by sending signaling messages to fibroblast cells. Neither ingredient is universally better. Each has a meaningful place depending on your skin type, tolerance, and goals.
If you layer actives with a daily SPF, which you absolutely should when using either of these ingredients, check the summer SPF upgrade guide for pairing recommendations. Below, we break down the science, the limitations, and the real-world tradeoffs so you can make an informed choice rather than a marketing-driven one.
Key Takeaways
- Retinol has stronger peer-reviewed evidence for reducing fine lines and increasing cell turnover, but research suggests up to 30% of users experience significant irritation, dryness, or barrier disruption during the adjustment period.
- Peptides such as palmitoyl tripeptide-1 and acetyl hexapeptide-3 may help support collagen synthesis and temporarily relax facial muscle contractions with far less risk of sensitivity, though long-term clinical data is thinner compared to retinoids.
- The FDA classifies retinol as a cosmetic ingredient, not a drug, at over-the-counter concentrations, but prescription-strength tretinoin (retinoic acid) is regulated separately and carries its own risk profile according to FDA guidance.
- Using peptides with retinol in a split routine (peptides in the morning, retinol at night) is widely supported by dermatologists as a complementary strategy rather than a competing one.
- Results vary significantly based on concentration, formulation stability, skin barrier health, and consistency of use. No topical ingredient can replicate the structural changes achieved by in-office procedures.
What Does Retinol Actually Do to Your Skin?
Retinol is a vitamin A derivative that converts to retinoic acid in the skin, where it binds to retinoid receptors and accelerates cell turnover while stimulating collagen production. It is one of the most studied topical anti-aging compounds available without a prescription.
When retinol (vitamin A, retinyl palmitate in stabilized ester form) is applied topically, it undergoes enzymatic conversion first to retinaldehyde, then to all-trans retinoic acid. That final compound is what actually binds to nuclear receptors and triggers gene expression changes that increase epidermal cell turnover and upregulate collagen synthesis in the dermis. This is why it works. It is also why it causes the notorious “retinization” period of flaking, redness, and tightness that derails so many routines.
What the Research Says About Retinol Efficacy
The American Academy of Dermatology includes topical retinoids in its evidence-based recommendations for improving the appearance of photoaged skin. Multiple controlled trials have documented measurable reductions in fine lines and improvements in skin texture after 12 to 24 weeks of consistent use. That said, most studies use prescription-strength tretinoin rather than cosmetic-grade retinol, and the conversion efficiency of over-the-counter retinol to active retinoic acid varies considerably depending on skin type, pH, and formulation.
Retinol Side Effects: Who Should Be Cautious?
Retinol side effects on skin are not just cosmetic inconveniences. The disruption to the skin barrier during early use can increase UV sensitivity, transepidermal water loss, and susceptibility to environmental irritants. People with rosacea, eczema, or a compromised moisture barrier may find that even low concentrations (0.025%) cause sustained inflammation rather than temporary adjustment. The FDA’s consumer guidance on retinoid safety specifically notes that all retinoids increase photosensitivity, making consistent broad-spectrum SPF use non-negotiable.
How Do Peptide Serums Work Differently?
Peptides are short amino acid chains that act as cellular messengers, signaling fibroblasts to produce more collagen or inhibiting neuromuscular communication to temporarily reduce expression lines. Their gentler mechanism makes them accessible to skin types that cannot tolerate retinol.
Peptide serum benefits come from a very different mechanism than the vitamin A pathway. Signal peptides like palmitoyl tripeptide-1 (Matrixyl) mimic the breakdown products of collagen, effectively tricking the skin into thinking it has sustained damage and needs to produce more collagen in response. Neurotransmitter-inhibiting peptides like acetyl hexapeptide-3 (Argireline) work more locally, limiting the acetylcholine release that drives repetitive muscle contractions at expression lines. Neither pathway involves the same receptor-level gene expression changes as retinoic acid, which is both their limitation and their strength.
What Peptides Cannot Do
Peptides have a meaningful research gap compared to retinoids. Many of the most-cited studies on compounds like palmitoyl pentapeptide-4 are sponsored by ingredient manufacturers such as Sederma, and independent, large-scale, double-blind trials are limited. Topical peptides also face a delivery challenge: most are hydrophilic (water-attracting) molecules that do not naturally penetrate the lipid-rich skin barrier efficiently without optimized carrier systems. A peptide serum sitting on top of the stratum corneum does far less than one formulated with encapsulation technology or lipopeptide modifications like the palmitoyl fatty acid attachments found in Matrixyl variants.
New Delivery Technologies Are Changing the Peptide Conversation
One of the biggest criticisms of topical peptides has always been their limited ability to penetrate the skin barrier. Because most peptides are relatively large, water-loving molecules, researchers have long questioned how much of an applied peptide actually reaches the deeper layers of the skin where collagen production occurs.
That challenge is beginning to change. Recent research published in 2025 highlights advances in cell-penetrating peptides (CPPs), cyclic peptides, and nanocarrier delivery systems designed to improve peptide stability, skin penetration, and targeted cellular uptake. These technologies aim to help peptides move through biological barriers more efficiently while protecting them from degradation before they reach their intended target.
A 2025 review published in Cosmetics noted that next-generation peptide formulations increasingly rely on advanced delivery platforms rather than peptide ingredients alone. Likewise, a 2025 review in Signal Transduction and Targeted Therapy identified delivery technologies as one of the most important factors driving the rapid evolution of peptide-based therapeutics and cosmetic applications.
While these innovations do not place peptides on equal scientific footing with retinoids yet, they may help close one of the largest performance gaps that has historically limited topical peptide efficacy. As a result, the peptide category in 2026 looks considerably more sophisticated than it did even a few years ago.

Peptides vs Retinol: Side-by-Side Comparison
Comparing these two ingredients across key performance and tolerance factors helps clarify which is better suited to different skin profiles and goals.
| Factor | Retinol | Peptides |
|---|---|---|
| Mechanism | Converts to retinoic acid, binds nuclear receptors, drives gene expression | Signals fibroblasts or inhibits neuromuscular activity via amino acid chains |
| Clinical Evidence Strength | Strong; multiple independent RCTs, AAD-endorsed | Moderate; many studies manufacturer-sponsored, fewer independent trials |
| Irritation Potential | High during adjustment; may cause peeling, redness, photosensitivity | Low; generally well-tolerated across sensitive and reactive skin types |
| Best For | Photoaging, texture, acne-prone skin, deeper lines with consistent use | Sensitive skin, expression lines, barrier-compromised skin, retinol alternatives |
| Pregnancy Safety | Not recommended; all retinoids are avoided during pregnancy per clinical guidelines | Generally considered safe; consult a dermatologist or OB-GYN to confirm |
| Stackability | Avoid with AHAs, BHAs, and benzoyl peroxide in same application; pH-sensitive | Compatible with most actives including niacinamide, hyaluronic acid, and SPF |
| INCI Examples | Retinol, Retinyl Palmitate, Retinaldehyde | Palmitoyl Tripeptide-1, Acetyl Hexapeptide-3, Palmitoyl Pentapeptide-4 |
Can You Use Peptides With Retinol?
Using peptides with retinol is not only possible but may offer complementary benefits, provided you separate them by time of day to avoid potential formulation conflicts and allow each ingredient to work at its optimal skin pH.
The short answer is yes, and many dermatologists suggest a split routine as one of the best anti-aging ingredient strategies available without a prescription. Retinol goes on at night, after skin is thoroughly cleansed and dry, to minimize irritation potential. Peptides work well in morning serums, where they pair naturally with hyaluronic acid (sodium hyaluronate), niacinamide, and broad-spectrum SPF. The pairing logic makes biological sense: retinol drives structural turnover overnight while peptides support signaling and hydration during the day.
One real formulation consideration is pH. Retinol performs best in formulations around pH 5.0 to 6.0. Some peptide serums are buffered to a higher pH for stability. Layering them in the same application can theoretically reduce the efficacy of both, which is why separation by routine, not just by minutes, tends to produce more consistent results for people who report the most improvement.
According to a 2019 study in the Journal of the American Academy of Dermatology (JAAD), topical retinoids demonstrated statistically significant improvements in fine lines and skin roughness versus vehicle control in subjects assessed over 24 weeks, with the majority of measurable benefit appearing after week 12.The National Institutes of Health (NIH) National Library of Medicine notes that signal peptides applied topically have shown measurable increases in types I and III procollagen in in-vitro and some in-vivo studies, though the authors of several reviewed papers acknowledge limitations including small sample sizes and lack of long-term follow-up data.
Alternative Perspectives
Some board-certified dermatologists argue that the marketing around peptide serums has significantly outpaced the evidence, and that consumers paying premium prices for peptide-forward formulas would see more measurable anti-aging results from consistent, low-dose retinol use over time. Their concern is that peptides offer a “feel-good” alternative that keeps people away from the one ingredient class with genuinely robust independent data.
On the other side, a growing number of cosmetic chemists and skin barrier researchers point out that chronic retinol-induced barrier disruption may actually accelerate certain signs of aging over time, particularly in dry or mature skin types where transepidermal water loss is already elevated. From this view, peptides are not a lesser substitute but a strategically smarter choice for a meaningful subset of the population.
There is also a cost-access dimension worth naming: effective retinol products are available at drugstore price points (retinyl palmitate formulas from brands like RoC or Neutrogena), while clinically meaningful peptide concentrations often appear in premium-priced serums. That pricing dynamic shapes who can access what, and it is worth considering when evaluating recommendations across beauty media.
Disclaimer
Results may vary. Product claims are based on available research and manufacturer information. This content is for informational purposes only and does not constitute medical or dermatological advice. Consult a licensed dermatologist for personalized skincare recommendations, particularly if you have a skin condition, are pregnant, or are considering prescription-strength retinoids.
Frequently Asked Questions
Is retinol or peptides better for sensitive skin?
Peptides are generally the better starting point for sensitive skin. Because they do not trigger the cell turnover acceleration that retinol initiates, they are far less likely to cause barrier disruption, redness, or peeling. People with rosacea or reactive skin may find that even low-concentration retinol formulas cause sustained irritation, while peptide serums, particularly those featuring palmitoyl tripeptide-1 or palmitoyl pentapeptide-4, tend to be well-tolerated. Results vary by individual, and a dermatologist consultation is the most reliable way to assess your specific tolerance.
Can you use peptides and retinol together in the same routine?
Yes, but most dermatologists suggest separating them by time of day rather than layering them in the same application. A common approach is applying a peptide serum in the morning alongside SPF, and reserving retinol for the nighttime routine. This avoids potential pH conflicts between formulations and allows each ingredient to function under its optimal skin conditions. Some users report that using a peptide moisturizer after retinol at night also helps buffer irritation during the adjustment period.
What are the most common retinol side effects on skin?
The most frequently reported retinol side effects include dryness, flaking, redness, and a tight or stinging sensation, particularly during the first four to eight weeks of use. These are often referred to collectively as the “retinization” period and may resolve as skin adjusts. More persistent concerns include increased photosensitivity, which makes daytime SPF use essential, and potential barrier disruption in people who already have dry or compromised skin. Starting with a low concentration (0.025% to 0.05%) used two to three nights per week is the approach most commonly recommended to minimize these effects.
Do peptide serums actually work for anti-aging?
Research suggests that certain peptides, particularly signal peptides like palmitoyl tripeptide-1 (Matrixyl) and carrier peptides, may support collagen synthesis and help improve the appearance of fine lines over time. However, the clinical evidence base is less robust than for retinoids, and many studies have been conducted by or in partnership with ingredient manufacturers. Independent, large-scale trials are limited. Peptides are most likely to show meaningful benefit when present in stable, well-formulated concentrations with appropriate delivery systems. Consumers should approach claims of “Botox-like” results from topical peptides with skepticism, as the mechanisms are not equivalent.



