GLP-1 receptor agonists like semaglutide (Ozempic, Wegovy) have reshaped how millions of Americans approach weight loss, but a critical finding from clinical research deserves serious attention: participants in the landmark STEP 1 trial published in The New England Journal of Medicine lost an average of 14.9% of their body weight, yet body composition sub-studies revealed that roughly 39% of that total weight loss came from lean mass rather than fat. That’s a significant portion of muscle walking out the door along with the fat, and the downstream consequences, including slower metabolism, reduced strength, and higher fall risk, can outlast the medication itself.
For the estimated 6 million Americans currently prescribed GLP-1 medications, this muscle-loss reality isn’t a reason to stop treatment. It’s a reason to pair treatment with the right fitness routines for beginners and advanced exercisers alike. The relationship between caloric restriction and lean tissue loss is well-established in metabolic research, and GLP-1-induced appetite suppression creates exactly the kind of prolonged caloric deficit that accelerates it. Structured exercise, particularly resistance training, is currently the strongest evidence-based tool available to counteract this process.
This guide covers what the research actually says about exercise on Ozempic, which types of movement matter most for muscle preservation, how to build a realistic workout plan for GLP-1 users, and where the current evidence still has gaps. For a broader look at the science behind these medications and other health articles on weight management, WideJournal’s health section covers the latest peer-reviewed findings.
Key Takeaways
- In the STEP 1 semaglutide trial, approximately 39% of total weight lost was lean mass, not fat, highlighting the real risk of muscle loss during GLP-1 therapy.
- Resistance training performed 2 to 3 times per week is the most evidence-supported strategy for preserving lean muscle mass during caloric restriction on GLP-1 medications.
- Protein intake of 1.2 to 1.6 grams per kilogram of body weight per day is recommended by sports nutrition researchers to support muscle retention during significant caloric deficits.
- GLP-1 users may experience reduced energy and nausea, especially early in treatment, making low-intensity exercise like walking a practical starting point before progressing to strength training.
- Current clinical guidelines from major health organizations do not yet include GLP-1-specific exercise protocols, meaning most recommendations are extrapolated from general caloric restriction research.
Why Muscle Loss on Wegovy and Ozempic Is a Real Clinical Concern
GLP-1 medications suppress appetite so effectively that users often eat far less protein and overall calories than their bodies need to maintain muscle, making structured resistance exercise essential rather than optional.
When the body is in a sustained caloric deficit, it draws energy from both stored fat and muscle protein. This process, known as lean mass catabolism, accelerates when protein intake drops below maintenance thresholds. GLP-1 receptor agonists work partly by slowing gastric emptying and reducing hunger signals in the brain, which means many users naturally eat smaller portions and, critically, often consume less protein than their muscles require to rebuild after daily activity.
What the Clinical Data Shows on Lean Mass Loss
The STEP 1 trial, one of the landmark studies on semaglutide 2.4 mg (Wegovy), measured body composition using DEXA scans alongside total weight loss. Participants who lost an average of 15.3 kg saw roughly 6 kg of that come from lean tissue. A 2022 post-hoc analysis published in Diabetes, Obesity and Metabolism noted that lean mass loss ratios on GLP-1 therapy are comparable to those seen with very low-calorie diets, which have long been associated with muscle depletion. This matters because muscle tissue is metabolically active: losing it lowers resting metabolic rate, making long-term weight maintenance harder and weight regain more likely once medication is stopped.
Who Is Most at Risk?
Older adults over 60 face the highest risk of clinically significant muscle loss on GLP-1 medications because age-related muscle decline (sarcopenia) is already underway before treatment begins. People who are sedentary at baseline, who have low baseline muscle mass, or who are losing weight very rapidly are also at elevated risk. Individuals with type 2 diabetes using semaglutide (Ozempic at lower doses) may have additional metabolic factors affecting protein synthesis. The limitation here is notable: most GLP-1 body composition studies have not stratified outcomes by exercise status at enrollment, so the true protective effect of pre-existing exercise habits isn’t yet fully quantified.
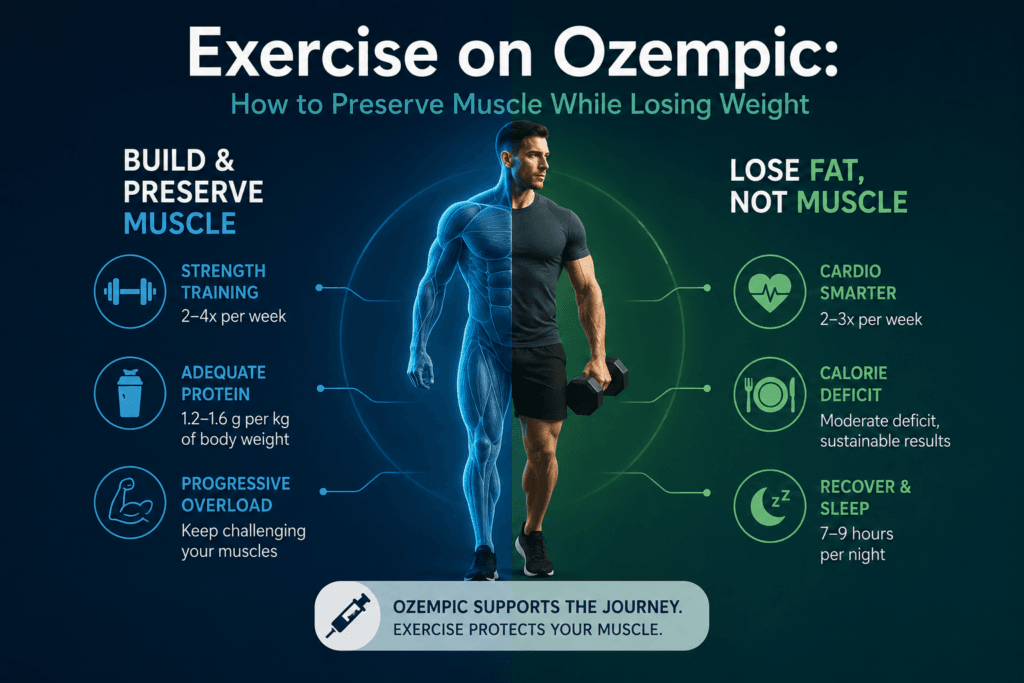
What Does a Workout Plan for GLP-1 Users Actually Look Like?
An effective workout plan for GLP-1 users prioritizes resistance training two to three times per week, adds low-impact cardio for cardiovascular health, and adjusts intensity based on energy availability and gastrointestinal side effects common early in treatment.
Resistance Training: The Non-Negotiable Foundation
Research consistently identifies progressive resistance training as the primary tool for preserving lean mass during caloric restriction. A meta-analysis of 66 randomized controlled trials, published in Obesity Reviews, found that resistance training during a caloric deficit reduced lean mass loss by approximately 80% compared to diet alone.
For GLP-1 users, this translates to a practical prescription: two to three sessions per week targeting all major muscle groups. However, because rapid weight loss often occurs in individuals starting with a high body mass, traditional barbell exercises can place excessive, dangerous sheer force on compromised knee, hip, and lower back joints.
To prevent joint degradation while maximizing muscle retention, exercises must be adapted based on your current mobility and baseline weight.
CRITICAL JOINT SAFETY STEP: If you have an elevated BMI, history of osteoarthritis, or joint pain, avoid free-weight compound movements (like standard barbell squats or walking lunges) until your weight stabilizes and baseline strength is established. Utilize closed-kinetic-chain machine exercises or bodyweight regressions that isolate muscles without overloading articular cartilage.
The Joint-Friendly GLP-1 Strength Framework
Instead of a rigid, one-size-fits-all routine, use this scaled approach to match your orthopedic reality:
| Target Area | Option A: Joint-Friendly / Beginner (Lower Joint Stress) | Option B: Progressive / Advanced (Higher Axial Loading) |
| Lower Body (Quad Dominant) | Leg Press Machine or Box Squats (sitting back onto a chair to limit knee shearing) | Barbell Back Squats or Goblet Squats |
| Lower Body (Posterior Chain) | Glute Bridges (bodyweight/banded) or Seated Leg Curls | Romanian Deadlifts (RDLs) or Kettlebell Swings |
| Upper Body Push | Chest Press Machine or Incline Dumbbell Press | Flat Barbell Bench Press or Overhead Press |
| Upper Body Pull | Seated Cable Rows or Lat Pulldowns | Bent-Over Barbell Rows or Pull-Ups |
| Core & Stability | Deadbugs or Bird-Dogs (zero spinal loading) | Standard Planks or Farmer’s Carries |
Parameters for Safety and Retention:
- Volume: Aim for 3 sets of 8 to 12 repetitions per exercise.
- Intensity: Choose a weight where the last 2 repetitions feel challenging but do not cause your form to break down.
- Rest: Take 60 to 90 seconds of rest between sets to support recovery, especially if you are experiencing GLP-1-induced fatigue.
Should You Do Cardio While on Semaglutide?
Cardiovascular exercise remains important for heart health, insulin sensitivity, and mood, but its role in muscle preservation is secondary to resistance work. The American College of Sports Medicine recommends at least 150 minutes of moderate-intensity cardio per week for adults managing weight. For GLP-1 users, low-impact options like brisk walking, cycling, or swimming are preferable early in treatment when nausea and reduced energy are common. High-intensity interval training (HIIT) can be incorporated once gastrointestinal side effects stabilize, typically after 8 to 12 weeks of dose titration.
Adjusting Exercise Intensity Around Side Effects
Up to 44% of participants in semaglutide trials reported nausea, and approximately 25% reported fatigue, particularly during dose escalation phases. Exercising through significant nausea risks dehydration and poor performance, which can reduce the quality of resistance sessions enough to negate their muscle-preserving benefit. A practical approach is to schedule resistance training on days when nausea is lowest, often 2 to 3 days after an injection for weekly-dosed medications, and to treat walking or light mobility work as the fallback on high-symptom days. This is not a failure of discipline; it’s appropriate self-regulation based on physiological reality.
Strength Training While on Semaglutide: Protein and Recovery Considerations
Protein intake and sleep quality are the two recovery variables most directly linked to muscle protein synthesis, and both are frequently disrupted in GLP-1 users eating significantly less food overall.
How Much Protein Do GLP-1 Users Need?
The current Recommended Dietary Allowance (RDA) for protein is 0.8 grams per kilogram of body weight per day, but this figure was established for sedentary adults maintaining weight, not individuals in a caloric deficit doing resistance training. Sports nutrition researchers, including those in the landmark International Society of Sports Nutrition (JISSN) Position Stand on protein and exercise, demonstrate that higher protein intakes are necessary to maximize the retention of lean body mass during hypocaloric (caloric deficit) periods. They recommend a scaled baseline that translates to roughly 1.2 to 1.6 grams per kilogram per day for individuals combining lifestyle interventions with significant weight loss. For a 200-pound (91 kg) person, that means aiming for 109 to 145 grams of protein daily. Given that GLP-1 users are eating less volume overall, hitting these targets requires deliberate food choices: prioritizing eggs, chicken, Greek yogurt, cottage cheese, and legumes before filling calories with lower-protein foods.
Sleep, Cortisol, and Muscle Repair on GLP-1 Therapy
Sleep deprivation elevates cortisol, a catabolic hormone that breaks down muscle tissue. Research suggests that less than 6 hours of sleep per night can reduce muscle protein synthesis by up to 18%, compounding the lean mass loss already occurring from caloric restriction. GLP-1 users who are losing weight rapidly may experience changes in sleep quality related to shifting body composition or metabolic changes, making sleep hygiene an underappreciated component of any muscle-preservation strategy.
GLP-1 Exercise Recommendations: Comparing the Evidence
No major clinical body has yet published GLP-1-specific exercise guidelines, so current recommendations are built from resistance training research in caloric restriction populations, with extrapolation to semaglutide therapy.
| Exercise Type | Frequency | Primary Benefit for GLP-1 Users | Evidence Level | Key Limitation |
|---|---|---|---|---|
| Progressive Resistance Training | 2-3x per week | Preserves lean muscle mass during caloric deficit | Strong (multiple RCTs) | Few studies conducted specifically in GLP-1 populations |
| Brisk Walking | Daily, 30+ minutes | Improves insulin sensitivity, manageable with nausea | Moderate | Minimal effect on lean mass preservation alone |
| High-Intensity Interval Training (HIIT) | 1-2x per week | Cardiovascular fitness, metabolic rate support | Moderate | Poorly tolerated during dose escalation phases |
| Yoga / Mobility Work | 2-3x per week | Stress reduction, cortisol management, flexibility | Limited for muscle preservation | Not sufficient as sole exercise modality |
| Swimming / Cycling | 2-3x per week | Low-impact cardio; joint-friendly for higher-weight users | Moderate | Less effective than resistance training for lean mass |
| Combined Resistance + Aerobic | 3-4x per week | Best overall body composition outcomes | Strong (meta-analytic support) | Higher time commitment; requires energy availability |
Alternative Perspectives
Not all researchers agree that muscle loss during GLP-1 therapy is a primary clinical concern requiring aggressive intervention. Some endocrinologists argue that the cardiovascular and metabolic benefits of rapid weight loss on semaglutide, including improved HbA1c, blood pressure normalization, and reduced liver fat, outweigh the risks of moderate lean mass reduction for most patients. In this view, prescribed exercise is beneficial but should not be framed as mandatory or guilt-inducing for patients who are physically limited or in early treatment phases.
A separate perspective comes from geriatric medicine specialists who note that for older adults or those with mobility limitations, high-intensity resistance training carries injury risk that must be weighed against its muscle-preserving benefits. Low-load, high-repetition resistance work and bodyweight exercises may provide meaningful muscle stimulus with lower injury risk for this population, though direct evidence in GLP-1 users is currently lacking.
There is also emerging debate about whether newer dual and triple agonist medications (like tirzepatide) may have different lean mass profiles than semaglutide alone, with some early trial data suggesting more favorable fat-to-lean loss ratios. The exercise implications of these differences are not yet established.
According to a 2021 study in Obesity Reviews (a meta-analysis of 66 RCTs with over 3,000 participants), combining resistance training with a caloric deficit preserved significantly more lean mass than diet restriction alone, with resistance training groups retaining approximately 80% more lean tissue over the intervention period.
According to the NIH National Institute on Aging, sarcopenia affects an estimated 10 to 16% of older adults globally, and any intervention that accelerates lean mass loss in this population, including significant caloric restriction without exercise, warrants proactive clinical attention.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making any health-related decisions. Individual results may vary.
Frequently Asked Questions
Can you build muscle while taking Ozempic or Wegovy?
Research suggests it is possible to maintain or modestly increase muscle mass while on semaglutide if resistance training is performed consistently and protein intake is adequate. However, building significant new muscle in a caloric deficit is physiologically difficult regardless of medication status. The more realistic and clinically meaningful goal for most GLP-1 users is preservation of existing lean tissue, not hypertrophy.
How soon after starting a GLP-1 medication should you begin exercising?
Walking and light movement can begin immediately. Structured resistance training is generally advisable once the initial nausea and fatigue of dose titration stabilize, which for many users occurs within the first 4 to 8 weeks of treatment. Anyone with cardiovascular disease, orthopedic limitations, or other complicating conditions should get clearance from their prescribing physician before starting a new exercise program.
Does exercise change how well GLP-1 medications work for weight loss?
Exercise does not appear to reduce the appetite-suppressing or weight-loss effectiveness of GLP-1 medications. Some studies on combined lifestyle and pharmacological interventions suggest that exercise may slightly enhance total weight loss outcomes. More importantly, exercise significantly improves the quality of that weight loss by shifting the fat-to-muscle ratio in a favorable direction, which has long-term metabolic consequences independent of the number on the scale.
What if fatigue and nausea make it hard to exercise on semaglutide?
Side effects are real and should not be dismissed. During high-symptom periods, even 10 to 15 minutes of bodyweight movements or a short walk maintains some neuromuscular stimulus without overtaxing the body. Many users find symptoms improve substantially after the dose stabilizes. Tracking injection days relative to symptom patterns can help identify optimal exercise windows. Persistent severe side effects that prevent any physical activity should be discussed with the prescribing provider.